Himanshu Arora, PhD
Founder & Chief Executive Officer
Computational pathology and translational AI researcher focused on uncertainty-aware diagnostic systems and multi-modal oncology infrastructure.
PathMDAi is a clinical intelligence layer for prostate cancer diagnosis — built for the disagreement zones where the field already disagrees with itself. Not a model. Not a dashboard. A second layer.
We don’t replace the pathologist’s eye. We hand them a second one, trained on the molecular layer they can’t see.— Founding thesis · 2024
Inter-pathologist disagreement on prostate Gleason 3 versus 4 routinely runs above thirty percent. That single gap drives over- and under-treatment, biopsy re-reads, and the slow, costly tail of clinical uncertainty.
PathMDAi does not compete with the pathologist’s sign-out. It illuminates the regions where the field already disagrees with itself, and gives the reviewer a structured second opinion — with confidence, evidence, and the tiles that produced each call.
The visual difference between pattern 3 and 4 is the presence of glandular boundaries. The transition is the single most consequential — and most disputed — call in prostate pathology.
~30%inter-rater disagreement · 3 ↔ 4Computational pathology has a credibility problem because the category over-promised. Our position is defined as much by what we refuse to be as by what we build.
No feature grid. No dashboard tour. The intelligence layer is a single workflow — five steps, every one auditable, every one keeping the pathologist in command.
H&E whole-slide images are normalized for stain, scanner, and institution drift before any inference runs. Architected for future LIS interoperability — not yet integrated.
The model surfaces the regions where field consensus historically breaks down — not where it is most confident, but where pathologists most need a second look.
Every flag is reviewable, overridable, and traceable. The co-pilot defers to the sign-out. Modifications are first-class objects in the report — not asterisks.
Confidence, evidence strength, and the tiles used to derive each call are recorded as structured metadata — readable by a reviewer, an auditor, and a regulator.
The pathologist retains final authority. The layer supports — never supplants — the review. What remains is a more confident report and an audit trail a regulator can read.
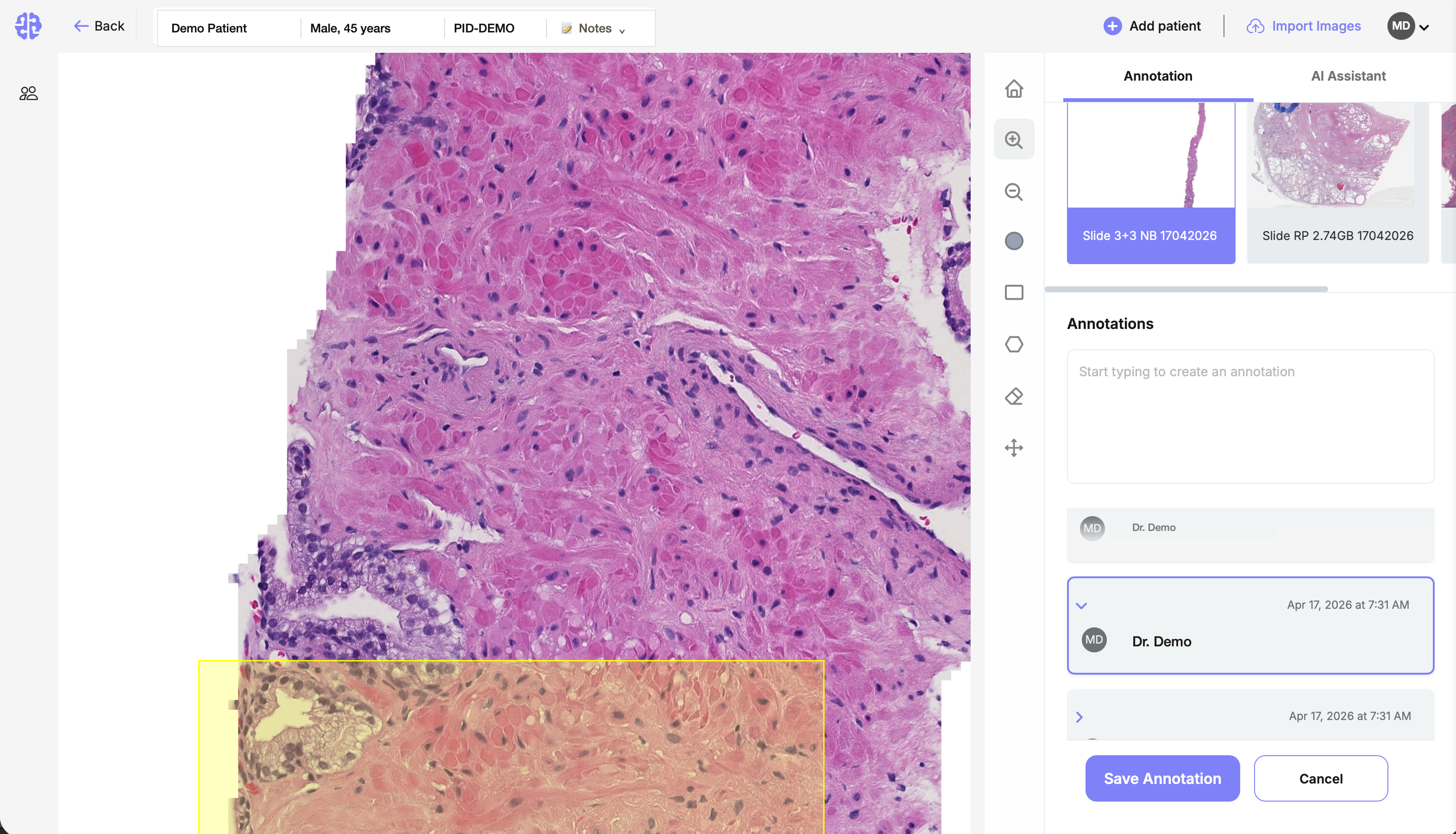
The five-step pipeline lives inside a single surface. Whole-slide field on the left, multi-block carousel and structured annotations on the right, AI Assistant a tab away. The pathologist controls every call.
Five forces are converging in the same window. Pathology AI is no longer a research curiosity — it is the operating layer the next decade of oncology will be built on.
Our grading model was characterized for bias and generalizability in npj Precision Oncology before a single hospital deployed it. Read the work, then read the pitch.
A research-led group of computational pathology operators, clinical leadership, and translational collaborators. Treated as a masthead, not a culture page.
Computational pathology and translational AI researcher focused on uncertainty-aware diagnostic systems and multi-modal oncology infrastructure.
Health-tech operator focused on capital strategy, regulatory finance, and institutional partnerships.
Computational biologist and bioinformatics researcher leading data strategy, validation, and model development.
Leads platform engineering, infrastructure architecture, and deployment systems for PathMDAi.
Leads pathology workflow integration, clinical evaluation, and pathologist-facing AI review strategy.
Supports pathology evaluation workflows and clinical review integration for validation-stage deployments.
Principal investigator focused on methodological rigor, translational research, and publication strategy.
Research collaborator focused on translational imaging systems and computational medicine.
Clinical collaborator supporting translational evaluation and future validation discussions in genitourinary oncology.
An intelligence layer is judged by what it does the day after the demo ends. Six commitments make PathMDAi a system a hospital’s legal, IT, and clinical leadership can sign for.
Designed with institutional deployment in mind. The data model and review surface are shaped to drop into existing pathology workflows when integration work begins. Not yet integrated.
The architecture trains where the data lives. PHI is not designed to leave the institution’s perimeter. HIPAA-aligned by construction.
Confidence, evidence strength, and the regions used to derive every output are stored as structured records — readable by a regulator, a reviewer, and a malpractice attorney.
Every flag is overridable. Every override is logged. The sign-out belongs to the human, full stop.
Each output is tied to the cohorts, model versions, and tile-level evidence that produced it. Versioning is a first-class concern, not a release note.
Every output is provisional until a pathologist signs. Modifications, overrides, and second-reads are first-class objects in the report — not asterisks.
We do not pretend to be further along than we are. The candor is the moat.
We publish what we get wrong.
Most AI vendors ship accuracy claims and a license agreement. We characterize our failure modes in peer review before we ask a hospital to deploy. That is the credibility bar regulators, payers, and senior pathologists actually use.
— Identity · operating principle 01Seed A is open. Use of proceeds: take the prostate co-pilot through FDA submission, add a third validating institution, and harden the federated deployment surface. Memo, cohort, and product walkthrough are shared with qualified investors after a fifteen-minute call.